
Why do I have tendon pain? What is Tendinitis versus Tendinopathy?
Oct 25, 2023
At the Digital Academy for Musculoskeletal Empowerment, our mission is to empower highly motivated, active individuals with knowledge on their journey to healing and recovery from musculoskeletal injuries.
Steven Makovitch DO and Christine Eng MD
Objectives:
- To describe why people get pain in their tendons (HINT: It is not just from inflammation like most people assume)
- To do this we will have to
- Define Tendinopathy: Explain what tendinopathy is and how it differs from historically used terms like "tendinitis" and "tendinosis."
- Describe Tendon Structure: Describe the composition of tendons, which are primarily made of collagen, and the role of tenocytes in maintaining tendon structure in response to mechanical load.
- Discuss Tendinopathy Development: Explain how tendinopathy develops due to trauma or altered loading, leading to degeneration and an imbalance in the tendon's healing process
- Identify Common Sites of Tendinopathy, Symptoms, and Risk Factors
Give me the Easy Version…
Tendons are tissues that connect muscles to bones and are crucial for movement and posture. “Itis” is the latin suffix which typically means inflammation. So, tendinitis literally translates to inflammation of a tendon. Tendinopathy is a condition that causes pain and impaired performance in a tendon. Since we now know that pain from a tendon is not really from just inflammation, tendinopathy is a preferred term used to describe this condition and has largely replaced the more commonly known "tendinitis".
Tendons are mainly made of collagen, which makes up about 60-85% of their dry weight. They also contain other components like proteoglycans, glycosaminoglycans, and glycoproteins. Tenocytes are the cells found in tendons that regulate the tendon's structure in response to mechanical load.
Tendinopathy can occur when a tendon undergoes repetitive trauma or altered loading, leading to degeneration and an imbalance in the tendon's healing process. The exact mechanisms are not fully understood, but repetitive overloading or underloading can contribute to its development.
Tendinopathy is prevalent in both athletes and the general population, with higher rates in females and older individuals. Common sites include the Achilles tendon, gluteal tendons, rotator cuff tendons, and elbow tendons (tennis and golfer’s elbow).
Symptoms of tendinopathy include pain, tenderness, difficulty with certain movements depending on the tendon affected. Diagnosis is usually based on a thorough history and physical examination, while imaging techniques like X-ray, MRI, and ultrasound can be helpful in some cases.
Give me the details…Deeper dive
First, some definitions below as a painful tendon can be described in many ways.
Tendinitis: Historically the term used for a painful tendon and the term still used by most of the lay public. This term has fallen out of favor over the years because most patients do not present with acute inflammation of a tendon- meaning, swelling, redness, warmth, with a significant amount of inflammatory cells at the microscopic level 1.
Tendinosis- diagnostic label for tendon pathology at the microscopic level that is degenerative with or without inflammation
Tendinopathy - used to signify a combination of pain and impaired performance associated with a tendon 2.
Tendinopathy is preferred term, to indicate a clinical diagnosis without knowing the specific mechanism or underlying tendon pathology.
Next, before we get into the abnormal, we must have a basic understanding of normal.
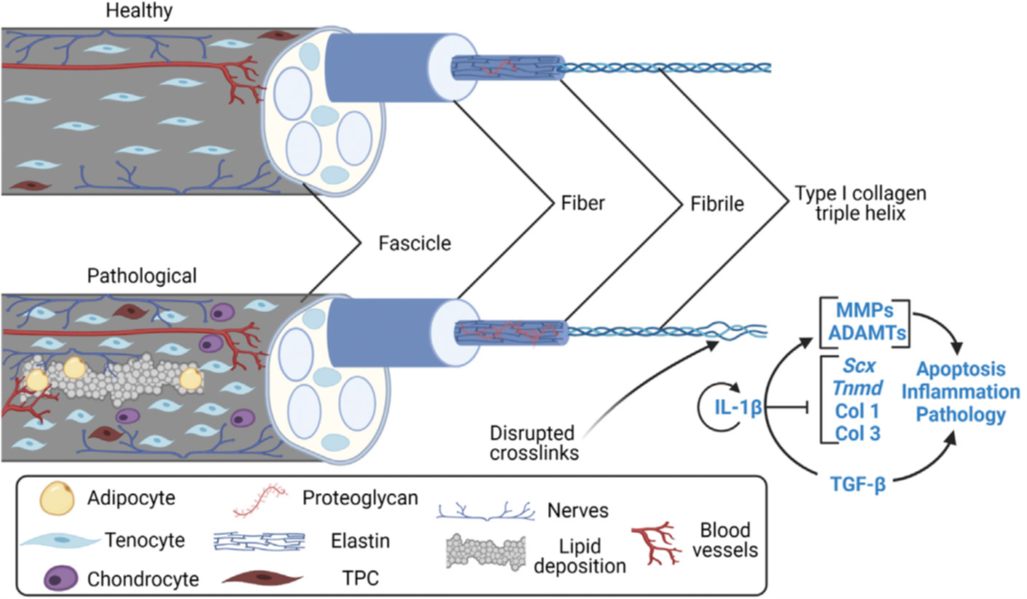
Think of tendons like a rope that connects a muscle to bone. When the muscle contracts it pulls on the rope that moves the bone. Tendons are made of a unique form of mechanosensitive connective tissue that transmits muscle contractile force to the boney skeleton to produce motion and maintain posture. Tendons are composed of triple-helical type I collagen molecules assembled into fibrils that, in turn, form fibers, fascicles, and ultimately, tendon 3(see healthy tendon image below).
Type I collagen accounts for about 60-85% of the dry weight of tendons. The remainder is composed of proteoglycans, glycosaminoglycans, glycoproteins, and collagen types III, XII, V. The actual tendon cells are called tenocytes and are uniformly aligned between collagen fibrils 3. Tenocytes are the predominant cell-type in a mature tendon and compose up 90–95% of actual cells, but only 5% of total tendon tissue volume 4. These tenocytes react to mechanical load (mechanotransduction) to regulate the synthesis and turnover of the tendon’s extracellular matrix components 5. Additionally, tendon stem/progenitor cells (TSPCs), also commonly called tendon-derived stem cells (TDSCs) or tendon stem cells (TSCs), located in the extracellular matrix, are responsible for replacing tendon cells through differentiation and proliferation 3.
Tendinopathy happens when a tendon undergoes some sort of trauma/overload which leads to a progressively degenerative imbalance in extracellular matrix turnover. The exact mechanisms for this imbalance is stated to not be fully characterized and understood. However, repetitive overloading or even underloading of a tendon can contribute to tendinopathy development. So, think of this like that rope from before has been used, waterlogged and left out in the sun- the structure of the rope actually changes, swells, deforms and gets frayed. This is like a tendon which actually will look swollen. The fibers will be irregular and there will be microtears or fraying. It will also be mechanically weakened.
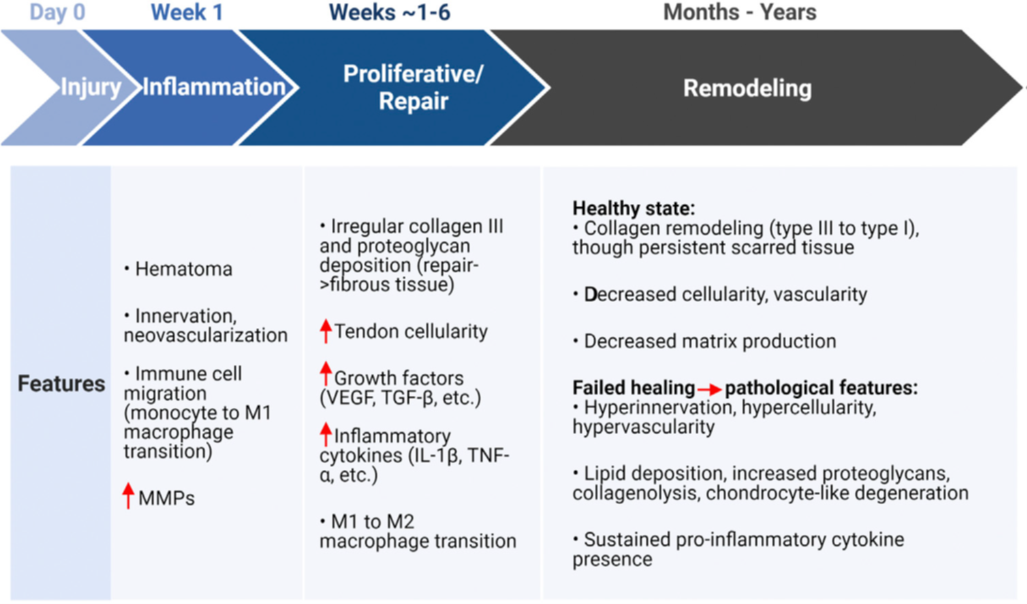
One of the most common classification systems related to tendinopathy is acute (0-6 weeks), sub-acute (6-12 weeks) and chronic tendinopathy (symptoms >3 months). When damage does occur to a tendon, there is a period of initial inflammation. There is molecular evidence to suggest that many of the key inflammatory interactions occur in the earlier stages of repetitive tendon microtrauma when patients may be asymptomatic. The tendon comes to a sort of crossroads between reparative versus degenerative healing 5.
Theories about the pathophysiology of tendinopathy are varied. Mechanisms include dysregulated apoptosis, mechanical overload, imbalance in the equilibrium between the activity of matrix metalloproteinases and tissue inhibitors of metalloproteinases, genetic factors (such as polymorphisms in COL5A1, neuronal proliferation and inflammation. At the pathological level we do know that there is the presence of neovascularization, apoptosis, lipid deposition, increased proteogylcans, sustained pro inflammatory cytokine presence, and an increased ratio of type III/type I collagen. Of note, Type III collagen is produced in the initial phases of tendon damage and is laid down haphazardly to try to patch things up and contributes to irregular alignment. Normally, type III collagen is slowly replaced by normal type I collagen, resuming a normal linear structural arrangement 5.
 Benage LG, Sweeney JD, Giers MB, Balasubramanian R. Dynamic Load Model Systems of Tendon Inflammation and Mechanobiology. Front Bioeng Biotechnol. 2022;10:896336.
Benage LG, Sweeney JD, Giers MB, Balasubramanian R. Dynamic Load Model Systems of Tendon Inflammation and Mechanobiology. Front Bioeng Biotechnol. 2022;10:896336.
Benage LG, Sweeney JD, Giers MB, Balasubramanian R. Dynamic Load Model Systems of Tendon Inflammation and Mechanobiology. Front Bioeng Biotechnol. 2022;10:896336.
How Common is Tendinopathy
Overall, tendinopathy is pretty common and you likely know someone with this condition. Also the overall prevalence of tendinopathy has been increasing. The prevalence of tendinopathy in general increases with age, and women are more affected than men. The incidence of tendinopathy in the lower extremities is 10.5 per 1000 persons and even exceeds that of osteoarthritis (8.4 per 1000) 6. In the lower extremity for the general population the most common sites with associated incidence rates are as follows: Gluteal tendinopathy (4%), patellar tendinopathy (1.6%), achilles tendinopathy (2.4%), and peroneal/posterior tibial tendinopathy (2.4%). However, rates can increase in certain situations. For example, the lifetime prevalence can increase to even greater than 50% in runners 7. In the upper extremity, common sites with associated prevalence rates include the rotator cuff (5.5%), and elbow with tennis elbow (0.7%) and golfers elbow (0.6%) 6.
What are risk factors for developing tendinopathy?
Some of the intrinsic risk factors for tendinopathy include systemic disease (diabetes, rheumatological inflammatory disorders), obesity, older age, hypermobility. Some extrinsic factors include overuse, sudden increase or change in activity level, inadequate time for recovery, poor ergonomics, medications including fluoroquinolones and statins 6. I would also add another risk factor with increasing studies that is not discussed enough yet is altered circadian biology or altered timing mechanisms (such as shift work, eating and staying up too late under artificial light, etc).
Clinically, what do we see with tendinopathy?
It largely depends on the tendon which is affected. Most of the diagnosis can come from a good history and physical examination. Those affected can have pain with specifically loading the tendon and have pain on palpation of the tendon. Imaging is not necessary for a diagnosis although can be helpful in certain situations by way of Xray, MRI and ultrasound.
Stay tuned for the treatment options…
- Alfredson H, Ljung BO, Thorsen K, Lorentzon R. In vivo investigation of ECRB tendons with microdialysis technique--no signs of inflammation but high amounts of glutamate in tennis elbow. Acta orthopaedica Scandinavica. 2000;71(5):475-479.
- Alfredson H. The chronic painful Achilles and patellar tendon: research on basic biology and treatment. Scandinavian journal of medicine & science in sports. 2005;15(4):252-259.
- Wang HN, Huang YC, Ni GX. Mechanotransduction of stem cells for tendon repair. World J Stem Cells. 2020;12(9):952-965.
- Benage LG, Sweeney JD, Giers MB, Balasubramanian R. Dynamic Load Model Systems of Tendon Inflammation and Mechanobiology. Front Bioeng Biotechnol. 2022;10:896336.
- Millar NL, Murrell GA, McInnes IB. Inflammatory mechanisms in tendinopathy - towards translation. Nature reviews Rheumatology. 2017;13(2):110-122.
- Millar NL, Silbernagel KG, Thorborg K, et al. Tendinopathy. Nat Rev Dis Primers. 2021;7(1):1.
- van der Vlist AC, Winters M, Weir A, et al. Which treatment is most effective for patients with Achilles tendinopathy? A living systematic review with network meta-analysis of 29 randomised controlled trials. British journal of sports medicine. 2021;55(5):249-256.
Do you feel like you want to know more, but don't know where to start? Join our course for Achilles tendinopathy to learn how to take charge of your own health!
Stay connected with news and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
We hate SPAM. We will never sell your information, for any reason.
